


Folate was first identified in the 1930s, where it was described as a ‘new haemopoietic factor’ found in yeast and liver, which was found to cure macrocytic anaemia. Further research in the 1940s resulted in the synthesis of pteroylglutamic acid from spinach, which was named folic acid after the Latin folium, meaning leaf.[1,2]
Folate is the general term used to describe a group of chemically similar forms of the water-soluble vitamin known as vitamin B9. Folate in food is known as pteroylpolyglutamate, with the richest sources including green leafy vegetables, sprouts, fruits, brewer’s yeast, liver and kidney.[3]
Folate is the general term used to describe a group of chemically similar forms of the water-soluble vitamin known as vitamin B9.
Dietary folates may be readily destroyed by cooking or processing, with a bioavailability approximately 40-50% less than that of synthetic folic acid.[4]
Folic acid is the form most commonly used in supplements and food fortification. Other supplemental forms of folate include folinic acid and 5-methyltetrahydrofolate (5-MTHF), both of which appear to have benefits over folic acid in terms of bioavailability and efficacy for certain individuals.
Through its role as a methyl donor, folate is involved in a range of biochemical reactions including neurotransmitter synthesis, DNA biosynthesis, regulation of gene expression, and amino acid synthesis and metabolism.[5]
Key Benefits
-
Important methyl donor
-
Supports homocysteine metabolism
-
Metabolism of amino acids
-
Involved in DNA and RNA synthesis
-
Involved in neurotransmitter synthesis
Clinical Applications
-
Alzheimer’s disease
-
Cognitive performance
-
Depression
-
Healthy methylation
-
Hyperhomocystaeinemia
-
Pregnancy – prevention of neural tube defects and health foetal development
-
Folate deficiency due to:
- inadequate dietary intake
- MTHFR gene polymorphisms
- malabsorption syndromes, e.g. coeliac and Crohn's disease
- long-term medication use, e.g. oral contraceptive pill, antacids, folate antagonists
- alcoholism
Mechanisms Of Action
Folate is an essential nutrient with its main biological action centering on its role as a methyl donor and its involvement in one-carbon metabolism, whereby folate coenzymes (or cosubstrates) accept or donate one-carbon units. Biochemical reactions dependant on folate coenzymes include DNA and RNA synthesis, amino acid metabolism and neurotransmitter synthesis.
DNA Synthesis
Folate coenzymes are involved in the synthesis of purines and pyrimidines that comprise DNA, making it essential for cellular division. Folate reduces damage to DNA, prevents replication errors, provides genomic stability and is involved in the repair of genetic material.[4,6] A deficiency of folate may be associated with disturbed cell cycling, cell apoptosis and increased rate of cell death.[4]
Amino Acid Metabolism
Folate is essential for the metabolism of several amino acids including methionine, cysteine, histidine, serine and glycine.[7] Folate, together with vitamin B12, is required for the metabolism of homocysteine through its remethylation into methionine. Low folate levels are associated with decreased synthesis of methionine and increased plasma homocysteine levels, which is a risk factor for atherosclerosis, recurrent thromboembolism, deep vein thrombosis, myocardial infarction, ischaemic stroke, dementia and cardiovascular disease mortality.[4,7]
Neurotransmitter Synthesis
Following the remethylation of methionine from homocysteine, the methyl group donated by folate allows for the conversion of methionine into S-adenosylmethionine (SAMe).[6] SAMe is subsequently able to function as a methyl donor in the synthesis of neurotransmitters including serotonin, dopamine, adrenaline, noradrenaline and histamine.[8] Folate deficiency is common in individuals with depression and is also associated with poor response to antidepressant treatment and relapse.[4,9] Supplemental folate is available in several forms including folic acid, folinic acid and 5-MTHF, each of which require varying degrees of metabolism and activation before they can be effectively utilised by the body as active folate.
Figure 1. Metabolic steps required for three forms of folic aciud to cross the blood-brain-barrier[9]
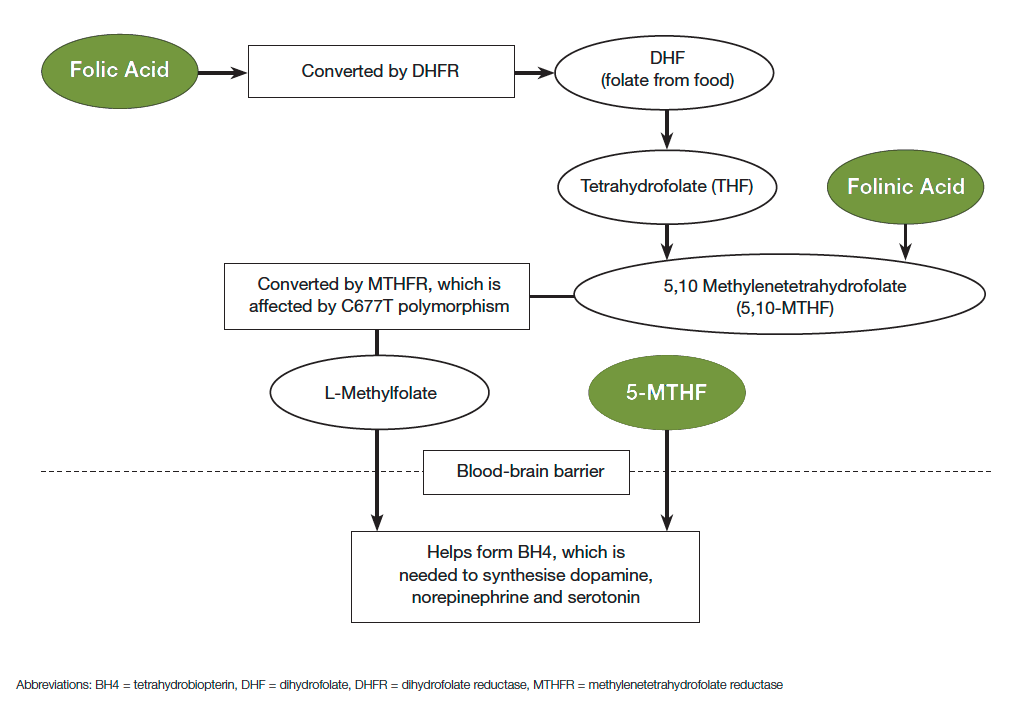
Folic Acid
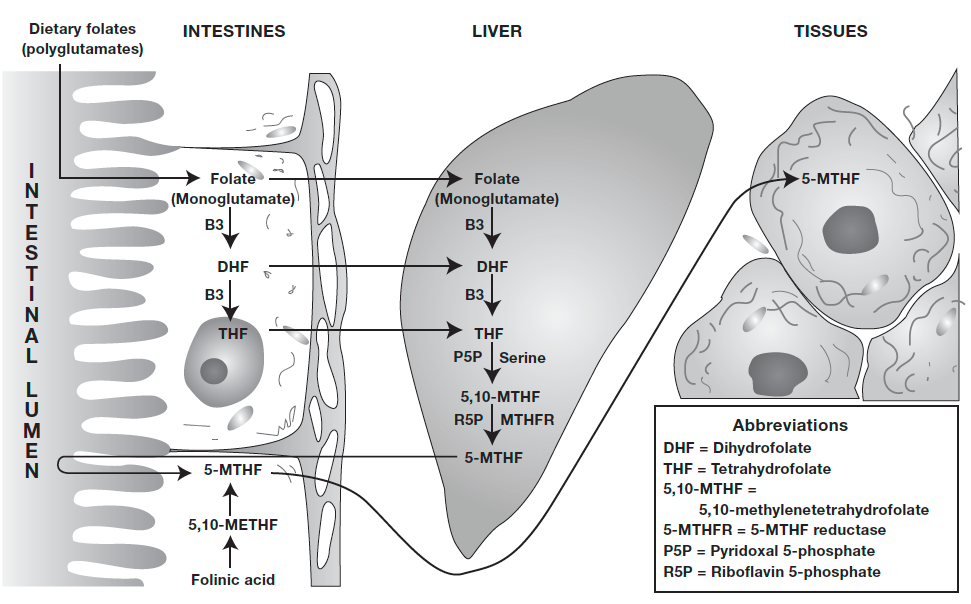
Folic acid is a synthetic, oxidised form of folate with a high degree of stability and an absorption rate of 85-95%, compared to 50% of folate from dietary sources.[5,10] It is widely used in supplements and fortified foods due to its stability, although it needs to be reduced intracellularly to tetrahydrofolate (THF) in order to become metabolically active.[11] The conversion process to the metabolically active coenzyme form of folate is complex and dependent on several enzymes including methylenetetrahydrofolate reductase (MTHFR) in addition to an adequate supply of nutrients including riboflavin (vitamin B2), niacin (vitamin B3), pyridoxine (vitamin B6), zinc and serine.[3]
Individuals with genetic polymorphisms of the MTHFR enzyme have varying degrees of impairment of folic acid metabolism, resulting in decreased production of the active form of folate, 5-MTHF.[5,11] Individuals with these genetic polymorphisms may benefit from supplemental 5-MTHF, thereby bypassing the steps required with folic acid supplementation.
Folinic Acid
Folinic acid appears to be a more metabolically active form of folate and is an immediate precursor to 5,10-methylenetetrahydrofolate (5,10-METHF), which in turn is rapidly metabolised to produce active folate (5-MTHF).[3]
Supplementation with folinic acid alleviates the need for the enzyme dihydrofolate reductase (DHFR) and bypasses the deconjugation and reduction steps that are required with folic acid supplementation. Bioavailability of folinic acid appears to be high, with human absorption studies showing a bioavailability of 92%.[12]
5-MTHF
5-methyltetrahydrofolate (5-MTHF) is the active form of folate and the major circulating form of folate in the body.7 5-MTHF is also the predominant type of folate found in food.[11]
5-MTHF does not require the enzymes methylenetetrahydrofolate reductase (MTHFR) or DHFR, and is able to cross the blood-brain barrier.
Individuals with MTHFR polymorphisms who have reduced capacity for producing 5-MTHF may benefit from 5-MTHF supplementation over folic acid supplementation. Research shows that supplementation with 5-MTHF increases blood folate levels equally to folic acid supplementation and may even be more effective.[10,13,14]
Supplementation with 5-MTHF is unlikely to mask the haematologic signs of vitamin B12 deficiency even at high intakes, which may occur with folic acid supplementation.[10]
Figure 1. Absorption and activation of folic acid
Clinical Studies
Folate improves symptoms of depression
Background: Folate is essential for the synthesis of noradrenaline, serotonin and dopamine, with a deficiency associated with depression, poor cognitive performance and reduced response to antidepressant medications.
Subjects/Method: Literature review.
Results: All three forms of supplemental folate – folic acid, folinic acid and 5-MTHF, appear to be well tolerated and efficacious for individuals with depression. Supplementation may enhance antidepressant medication efficacy and may convert nonresponders into responders.
Periconceptional folate prevents neural tube defects (NTDs)
Background: To examine the role of folate supplementation before and during early pregnancy in reducing neural tube and other birth defects without causing adverse outcomes for mothers or babies.
Subjects/Method: Scientific literature review involving 6105 women (1949 with a history of a pregnancy affected by a NTD and 4156 with no history of NTDs).
Results: Overall, the results showed a protective effect of daily folic acid supplementation in preventing NTDs, compared with no intervention or placebo. Folic acid had a significant protective effect for reoccurrence. The reviewers concluded that folic acid, alone or in combination with vitamins and minerals, is effective for the prevention of NTDs, although its effect on other birth defects is not clear.
Folic acid and L-MTHF reduce homocysteine levels
Background: Folic acid fortification may lower total homocysteine concentrations (tHcy), but may mask vitamin B12 deficiency. The L-5-methyltetrahydrofolate (L-MTHF) form of folic acid may provide the homocysteine-lowering benefits of folate, without masking the haematologic indicators of vitamin B12 deficiency.
Subjects/Method: Randomised double-blind, placebo-controlled trial involving 167 healthy participants.
Intervention: Trial participants received either 100mcg folic acid, 113mcg L-MTHF or placebo daily for 24 weeks.
Results: After 24 weeks supplementation, L-MTHF was found to be more effective than folic acid in lowering tHcy. Both folic acid and L-MTHF increased plasma folate and red blood cell folate concentrations.
Dosage Range For Conditions According To Clinical Studies
| Condition | Dosage | References |
| Preconception and early pregnancy | 400-800mcg/day (folate) | 6,15 |
| Preconception and early pregnancy in women with a previous NTD | 4-5mg/day (folate) | 6,15 |
| Cognitive decline | 800mcg/day (folic acid) | 16 |
| Depression | 2-50mg/day (5-MTHF) as stand-alone treatment 200-500mcg/day (folate) alongside antidepressants |
|
| Hyperhomocysteinaemia | 500-5000mcg/day (folate) | 6 |
| Methotrexate toxicity | ≥7mg/week (folic acid or folinic acid) | 17 |
| Oral contraceptive pill-induced folate deficiency | 2mg/day (folate) | 6 |
| Folate deficiency | 250mcg-5mg/day (folate) | 4,6 |
Cautions And Contraindications
- Folate supplementation may mask a vitamin B12 deficiency state. Folate and vitamin B12 deficiencies are both characterised by the same haematologic symptom, megaloblastic anaemia, which disappears with folate supplementation. This leaves the B12 deficiency to remain untreated and allows for the progression of neurological damage.[14] It is recommended that patients be screened for vitamin B12 deficiency.[6]
- Doses above 5mg per day may cause abdominal cramps, diarrhoea and skin rashes. Higher doses of 15mg per day may cause altered sleep patterns, irritability, excitability, overactivity, confusion, digestive disturbances and zinc depletion.[4]
- Folate supplementation may exacerbate seizures in patients with seizure disorders, although this is rare in doses less than 1000mcg.[4]
- Folate supplementation may reduce the efficacy of methotrexate prescribed for the treatment of acute lymphoblastic leukaemia. Theoretically, this may reduce its efficacy in the treatment of other cancers.[4] Note that folate supplementation is recommended for individuals prescribed methotrexate for rheumatoid arthritis or psoriasis, due to its beneficial effect in reducing methotrexate side-effects without reducing the efficacy of the drug itself.
Folic Acids Food Fortification
Mandatory folic acid food fortification has been implemented in a number of countries to reduce the occurrence of NTDs and associated morbidity and mortality. Although these fortification programs have proved successful in reducing the prevalence of NTDs, possible concerns have been raised. These include masking of B12 deficiency anaemia, promotion of cancer, changes in epigenetic patterns and increasing levels of circulating unmetabolised folic acid.[18,19]
Researchers have suggested that decisions regarding folic acid food fortification should take into account these potential concerns, with further pre-clinical and population-based studies warranted to minimise any future risk associated with mandatory folic acid food fortification.[20,21]
References
- Rosenberg IH. A history of the isolation and identification of folic acid (folate). Ann Nutr Metab 2012;61(3):231-235. [Abstract]
- Hoffbrand AV, Weir DG. The history of folic acid. Br J Haematol 2001;113(3):579-589. [Full text]
- Kelly GS. Folates: supplemental forms and therapeutic applications. Altern Med Rev 1998;3(3):208-220. [Abstract]
- Folic acid. Natural Medicine Comprehensive Database 2015, www.naturaldatabase.com
- Miller AL. The methylation, neurotransmitter, and antioxidant connections between folate and depression. Altern Med Rev 2008;13(3):216-226. [Full text]
- Braun L, Cohen M. Herbs and natural supplements: an evidence-based guide, 3rd ed. Sydney: Churchill Livingstone Elsevier, 2010.
- Higdon J. Folate. Micronutrient information center, Linus Pauling Institute 20007, http://lpi.oregonstate.edu/mic/vitamins/folate
- Bottiglieri T. S-Adenosyl-L-methionine (SAMe): from the bench to the bedside--molecular basis of a pleiotrophic molecule. Am J Clin Nutr 2002;76(5):1151S-1157S. [Full text]
- Fava M, Mischoulon D. Folate in depression: efficacy, safety, differences in formulations, and clinical issues. J Clin Psychiatry 2009;70 Suppl 5:12-17. [Abstract]
- Venn BJ, Green TJ, Moser R, et al. Increases in blood folate indices are similar in women of childbearing age supplemented with [6S]-5-methyltetrahydrofolate and folic acid. J Nutr 2002;132(11):3353-3355. [Full text]
- Prinz-Langenohl R, Brämswig S, Tobolski O, et al. [6S]-5-methyltetrahydrofolate increases plasma folate more effectively than folic acid in women with the homozygous or wild-type 677C-->T polymorphism of methylenetetrahydrofolate reductase. Br J Pharmacol 2009;158(8):2014-2021. [Full text]
- McGuire BW, Sia LL, Leese PT, et al. Pharmacokinetics of leucovorin calcium after intravenous, intramuscular, and oral administration. Clin Pharm 1988;7(1):52-58. [Abstract]
- Houghton LA, Sherwood KL, Pawlosky R, et al. [6S]-5-Methyltetrahydrofolate is at least as effective as folic acid in preventing a decline in blood folate concentrations during lactation. Am J Clin Nutr 2006;83(4):842-850. [Full text]
- Lamers Y, Prinz-Langenohl R, Brämswig S, et al. Red blood cell folate concentrations increase more after supplementation with [6S]-5-methyltetrahydrofolate than with folic acid in women of childbearing age. Am J Clin Nutr 2006;84(1):156-161. [Full text]
- De-Regil LM, Fernández-Gaxiola AC, Dowswell T, et al. Effects and safety of periconceptional folate supplementation for preventing birth defects. Cochrane Database Syst Rev 2010 Oct 6;(10):CD007950. [Full text]
- Durga J, van Boxtel MP, Schouten EG, et al. Effect of 3-year folic acid supplementation on cognitive function in older adults in the FACIT trial: a randomised, double blind, controlled trial. Lancet 2007;369(9557):208-216. [Abstract]
- Shea B, Swinden MV, Tanjong Ghogomu E, et al. Folic acid and folinic acid for reducing side effects in patients receiving methotrexate for rheumatoid arthritis. Cochrane Database Syst Rev 2013 May 31;5:CD000951. [Full text]
- Crider KS, Bailey LB, Berry RJ. Folic acid food fortification - its history, effect, concerns, and future directions. Nutrients 2011;3(3):370-384. [Full text]
- Mathers JC. Folate intake and bowel cancer risk. Genes Nutr 2009;4(3):173-178. [Full text]
- Kim YI. Folic acid fortification and supplementation--good for some but not so good for others. Nutr Rev 2007;65(11):504-511. [Abstract]
- Choi JH, Yates Z, Veysey M, et al. Contemporary issues surrounding folic acid fortification initiatives. Prev Nutr Food Sci 2014;19(4):247-260. [Full text]
DISCLAIMER:
The information provided on FX Medicine is for educational and informational purposes only. The information provided on this site is not, nor is it intended to be, a substitute for professional advice or care. Please seek the advice of a qualified health care professional in the event something you have read here raises questions or concerns regarding your health.
