

Histamine intolerance (HIT) continues to be a topic of in-creasing clinical interest with scientific research continuing into its prevalence, aetiology, pathophysiology, clinical presentation, and comorbidities along with the most appropriate therapeutic assessment and management strategies. There is significant complexity associated with each of these - paralleled by the ubiquitous physiological and functional nature of this biogenic amine in relation to the many body systems, organs and tissues it influences, as well as the interindividual variability in its clinical manifestation/presentation.2-4
Histaminosis
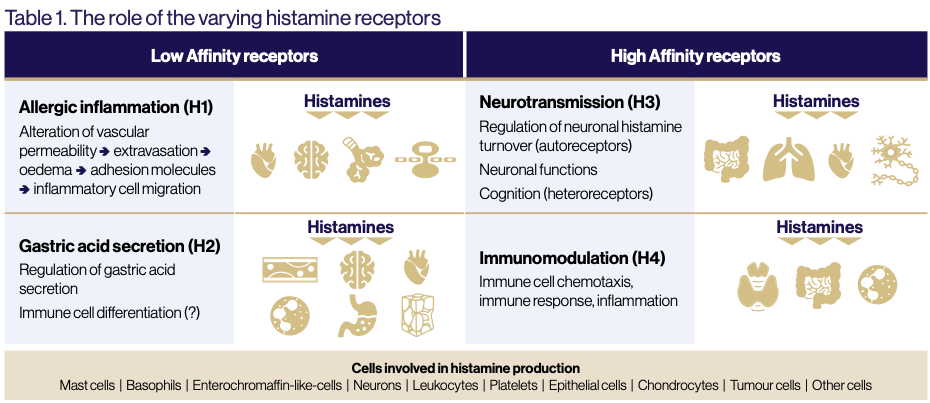
Histaminosis (HIT) is reported to affect up to 3% of the population, however, with its clinical heterogeneity and diagnostic challenges, its actual prevalence may be higher.5 -7 Histaminosis is defined as the impaired capacity to methylate/deaminate histamine via diamine oxidase (DAO) and histamine N-methyltransferase (HNMT) enzymes respectively. This inability results in the accumulation of endogenous histamine, allowing it to bind to histamine receptors (HR 1-4) producing subsequent effects on tissues and organs2,7,8,10 (See Table 1 and Histamine Basics).

Histamine Basics
Synthesis
Histamine is synthesised intracellularly in central and peripheral tissues in the Golgi apparatus organelle following decarboxylation of L-histidine by the inducible enzyme histidine decarboxylase.2,11 This occurs in cells that store histamine including mast cells and basophils, and cells that produce histamine in response to stimuli such as enterochromaffin-like, histaminergic neurons, lymphocytes, monocytes, platelets, neutrophils, gastric and dendritic cells.1,4,10 Such stimuli can involve both immunological and non-immunological substances.2
Function
Histamine is necessary in the body for many functional processes including:
• Inflammation
• Innate and adaptive immunity
• Vasodilation and vascular permeability
• Smooth muscle contraction and relaxation
• Gastric acid secretion
• Neuromodulation (including thermoregulation, appetite and cognition).1,3,9,11,12
Metabolism and Inactivation
Endogenous histamine is metabolised intracellularly by histamine N-methyltransferase (HNMT) (expressed in respiratory, small intestinal, liver and kidney cells) via deamination and extracellularly by diamine oxidase (DAO) through methylation.2,4,11,13 DAO, largely expressed by intestinal epithelial villi cells as well as liver, kidney, placental and skin cells, breaks down 15-30% of histamine by removing an amine group, producing imidazole acetaldehyde, ammonia and hydrogen peroxide. This pathway requires vitamins B6, C and copper to function effectively.4,8,11,13 Because HNMT is more widely expression throughout the body it metabolises 50-80% of endogenous histamine by adding a methyl group from S-adenosyl-L-methionine, producing N-methylhistamine and subsequently M-methylimidazole acetic acid.4,8,9
Causes of Histamine Intolerance (HIT)
The many endogenous and exogenous aetiological factors associated with HIT pathophysiology are clinically observed to predominantly involve multiple antecedents rather than an individual trigger.
Endogenous aetiologies of histamine intolerance include:
• Genetic (DAO rs10156191, rs1049742, rs2268999, and rs104979 polymorphisms)
• Acquired (functional) impairment of DAO or HNMT enzymes
• Gastrointestinal dysfunction or pathology (damaged intestinal enterocytes, bleeding, inflammation, dysbiosis and infections)
• Nutrient deficiencies (copper, vitamins C and B6).1-3, 6,8,10,11,13,15,16
Exogenous aetiologies of histamine intolerance include:
• Diet (considered to be a significant exogenous trigger) specifically the ingestion of foods with high levels of histamine (sauerkraut, processed meat, dried anchovies, fish sauce, spinach, tomatoes, cocoa, eggplant, fish, chicken, yoghurt, soy, red wine); those promoting mast cell histamine release (citrus foods, pineapple, bananas, strawberries, papaya, tomatoes, additives); or containing other biogenic amines that interfere with the binding of histamine to mucosal mucine resulting in more histamine in circulation.10,11,13,18
• Other exogenous factors include stress, alcohol, medications and xenobiotics that decrease DAO activity (or interfere with histamine metabolism and distribution).3,8,15,20
Symptoms of Histamine Intolerance
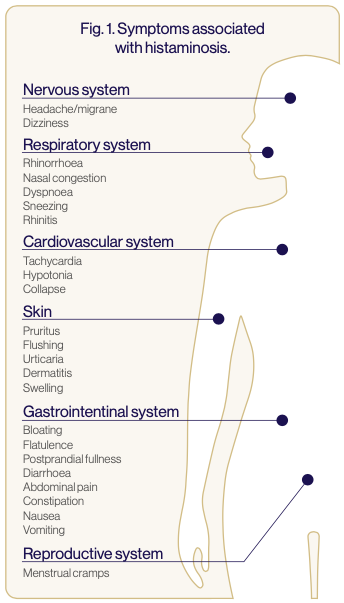
Histamine Intolerance results in the onset of a broad range of symptoms across different body systems. The more commonly observed symptoms in clinical and research settings are:
• Gastrointestinal (abdominal distension, constipation, postprandial fullness, nausea, vomiting, diarrhoea, abdominal pain and constipation)
• Nervous (dizziness, headaches and migraines)
• Respiratory (sneezing, rhinorrhoea, nasal congestion, swelling, phlegm, cough and asthma)
• Integumentary (eczema, dermatitis, urticaria, pruritis, flushing and oedema)
• Muscular (pain)
• Cardiovascular (tachycardia and hypotension)3,5-7,10,13-17
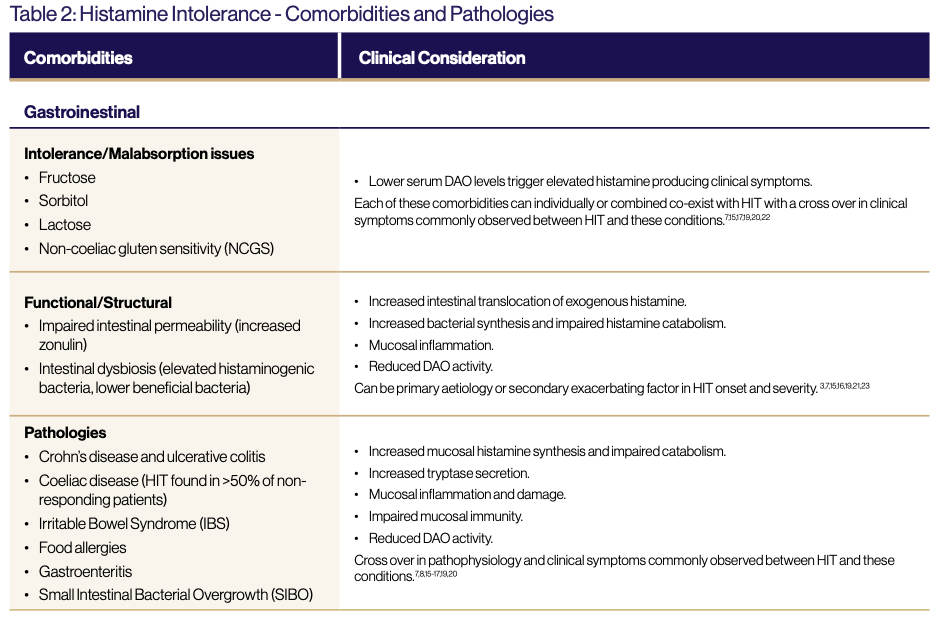
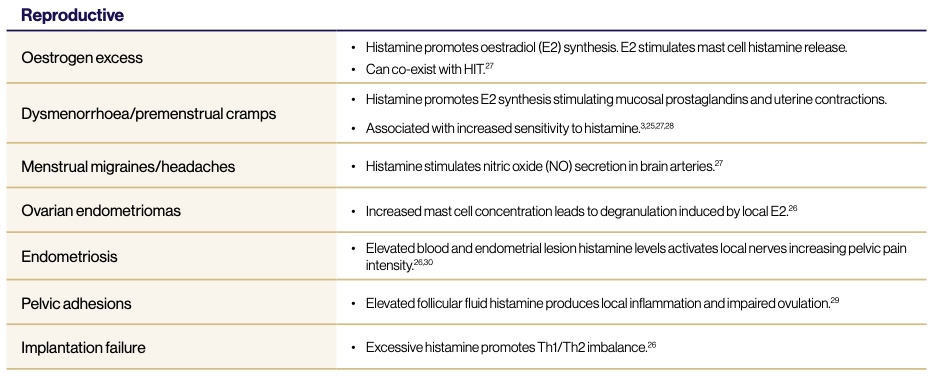
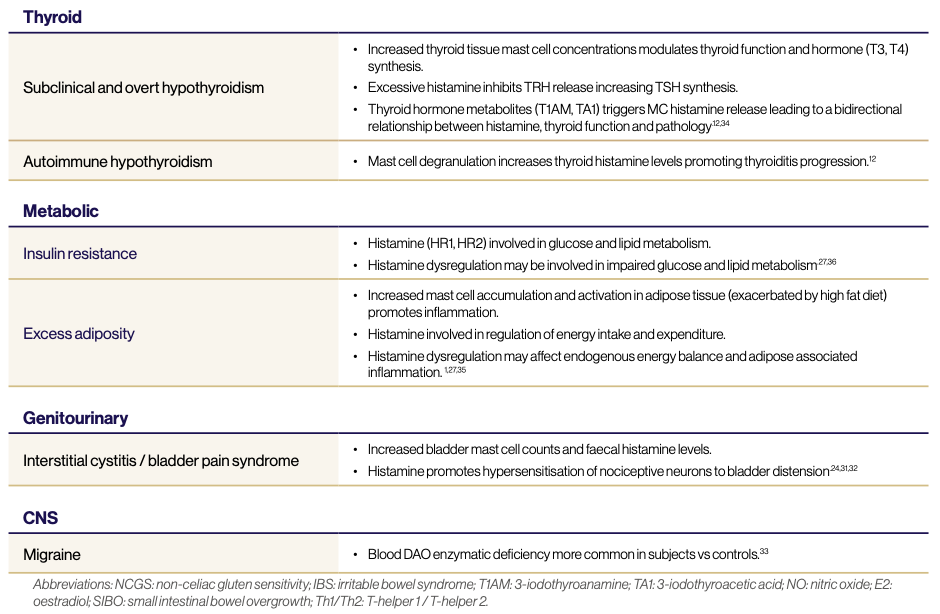
In addition to these more commonly observed clinical presentations of HIT, correlations between the condition and other clinical pathologies are emerging (See Fig. 1 and Table 2).
Clinical Assessment of Histamine Intolerance
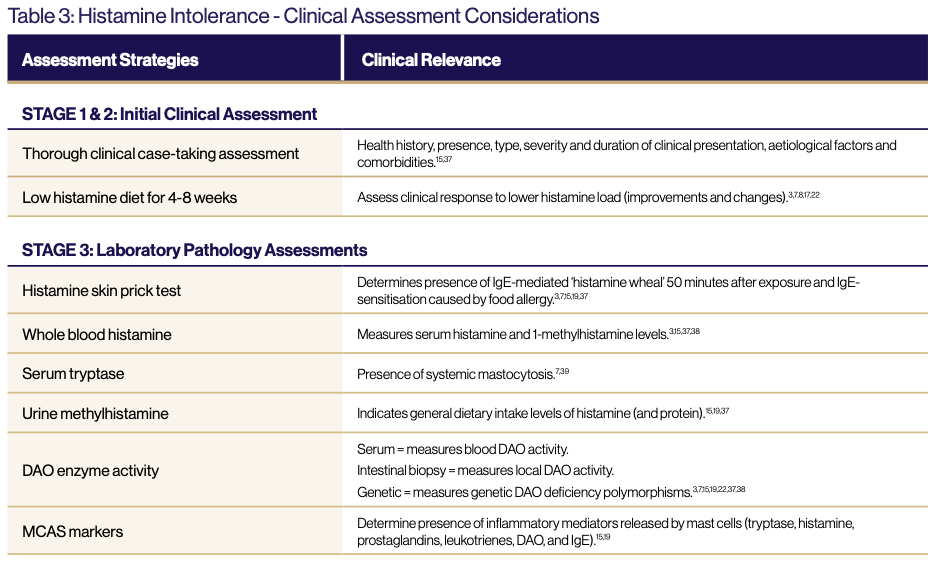
The heterogenous nature of the aetiology, pathophysiology and clinical presentation of HIT and the variability of the validity and clinical information provided by commonly utilised assessment strategies are essential considerations in the accurate clinical diagnosis and effective clinical management of HIT. (See Table 3.)
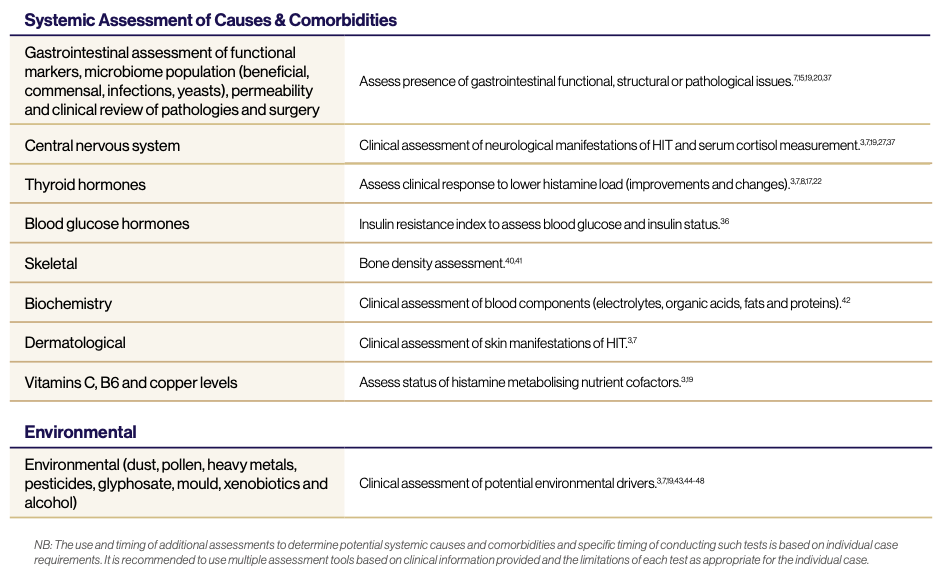
This review emphasises that the basis of effective clinical management of HIT is through the thorough assessment of the systemic clinical presentation and consideration of all potential aetiological and pathophysiological factors in the individual case, as well as the importance of ongoing research to improve the diagnosis and treatment of this condition.
Download a free copy of this article

References
1. Barcik W, Wawrzniak M, Akkis CA, O’Mahony L. Immune regulation by histamine and histamine-secreting bacteria. Curr Opin Immunol 2017; 48: 108-113.
2. Kyriakidis DA, Theodorou MC, Tiligada E. Histamine in two component system-mediated bacterial signaling. Front Biosci 2012 Jan; 17: 1108-1119.
3. Hrubisko H, Danis R, Huorka M, Wawruch M. Histamine intolerance – the more we know the less we know. A review. Nutrients 2021, 13(7): 2228, DOI: 10.3390/nu13072228.
4. Patel RH, Mohiuddin SS. Biochemistry, histamine. Treasure Island (FL): StatPearls Publishing, 2022.
5. Pinzer TC, Tietz E, Waldmann E, Schink M, Neurath MF, Zopf Y. Circa- dian profiling reveals higher histamine plasma levels and lower diamine oxidase serum activities in 24% of patients with suspect- ed histamine intolerance compared to food allergy and controls. Allergy 2018; 73(4): 949-957.
6. Cucca V, Ramirez GA, Pignatti P, Asperti C, Russo M, Della-Torre E et al. Basal serum diamine oxidase levels as a biomarker of histamine intolerance: a retrospective cohort study. Nutrients 2022; 14(7): 1513, DOI: 10.3390/nu14071513.
7. Comas-Baste O, Sanchez-Perez S, Veciana-Nogues MT, Latorre-Moratalla M, del Carmen Vidal-Carou M. Concept etiology and current diagnostic and treatment approaches of histamine intolerance: a review. In: Zepeda-Carillo E, editor. Prime Archives in Nutrition. Hyderabad, India: Vide Leaf, 2021.
8. Comas-Baste O, Sanchez-Perez S, Veciana-Nogues M, La- torre-Moratalla M, Vidal-Carou MDC. Histamine intolerance: the current state of the art. Biomolecules 2020; 10 (8): 1181, DOI: 10.3390/biom10081181.
9. Jones BL, Kearns GL. Histamine: new thoughts about a familiar mediator. Clin Pharm Ther 2011; 89 (2): 189-197.
10. Maintz L, Novak N. Histamine and histamine intolerance. Am J Clin Nutr 2007 May; 85 (5): 1185-96.
11. Schwelberger HG, Ahrens F, Fogel W, Sanchez-Jimenez F. His- tamine metabolism. In: Histamine H4 receptor: a novel drug target in immunoregulatory and inflammatory diseases (Ed. Stark H). 2013. Versita, London/UK.
12. Landucci E, Laurino A, Cinci L, Gencarelli M, Raimondi L. Thyroid hormone, thyroid hormone metabolites and mast cells: a less explored issue. Frontiers in Cellular Neuroscience 2019; 13: 79, DOI: 10.3389/fncel.2019.00079.
13. Kovacova-Hanuskova E, Buday T, Gaviakova S, Plevkova J. Histamine, histamine intoxication and intolerance. Allergol Immu- nolpathol (Madr). 2015; 43 (5): 498-506.
14. Reese I, Ballmer-Weber B, Beyer K, Fuchs T, Kleine-Tebbe J, Klimek L, Lepp U et al. German guideline for the management of adverse reactions to ingested histamine. Allergo J Int 2017; 26: 72-79. Zhao Y, Zhang X, Jin H, Chen L, Ji J, Zhang Z. Histamine intolerance – a kind of pseudoallergic reaction. Biomolecules 2022; 12(3): 454, DOI: 10.3390/biom12030454.
15. Zhao Y, Zhang X, Jin H, Chen L, Ji J, Zhang Z. Histamine intolerance – a kind of pseudoallergic reaction. Biomolecules 2022; 12(3): 454, DOI: 10.3390/biom12030454.
16. Sanchez-Perez S, Comas-Baste O, Duelo A, Veciana-Nogues MT, Berlanga M, Latorre-Moratalla ML et al. Intestinal dysbiosis in patients with histamine intolerance. Nutrients, 2022; 14(9): 1744, DOI: 10.3390/nu14091774.
17. Pinzer TC, Tietz E, Waldmann E, Schink M, Neurath MF, Zopf Y. Circa- dian profiling reveals higher histamine plasma levels and lower diamine oxidase serum activities in 24% of patients with suspect- ed histamine intolerance compared to food allergy and controls. Allergy, 2017; 73(4): 949-957.
18. Mauro Martin IS, Brachero S, Garicano Vilar E. Histamine intol- erance and dietary management: a complete review. Allergol Immunopathol (Madr). 2016; 44 (50: 475-483.
19. Shulpekova YO, Nechaev VM, Popova IR, Deeva TA, Kopylov AT, Malsagova K et al. Food intolerance: the role of histamine. Nutrients 2021; 3(9): 3207, DOI: 10.3390/nu1393207.
20. Schnedl WJ, Enko D. Histamine intolerance originates in the gut. Nutrients 2021; 13(4): 1262, DOI: 10.3390/nut13041262.
21. Hasler WL, Grabauskas G, Singh P, Owyang C. Mast cell mediation of visceral permeability in irritable bowel syndrome. Neurogastroenterology & Motility 2022; e14339, DOI: 10.1111/nmo.14339.
22. Schnedl WJ, Meier-Allard N, Michaelis S, Lackner S, Enko D, Mangge H et al. Serum diamine oxidase values, indicating histamine intolerance, influence lactose tolerance breath test results. Nutrients 2022; 14(10): 2026, DOI: 10.3390/nu14102026.
23. Schink M, Konturek PC, Tietz E, Dietrich W, Pinzer TC, Wirtz S et al. Microbial patterns in patients with histamine intolerance. Jour- nal of Physiology and Pharmacology 2018; 69(4), DOI: 10.26402/ jpp.2018.4.09.
24. van Thiel IAM, Botschuijver S, de Jonge WJ, Seppen J. Painful interactions: microbial compounds and visceral pain. Biochemica et Biophysica Acta (BBA) – Molecular Basis of Disease 2020; 1866 (1): 165534.
25. Noor N, Tripathi T, Moin S, Faizy AF. Possible effect of histamine in physiology of female reproductive function: an updated review. In: Biomedical Aspects of Histamine, Shahid M, editor. Springer Science Business Media BV, 2010, DOI: 10.1007/978-90-481-9349-3_18.
26. Komi DEA, Shafaghat F, Haidl G. Significance of mast cells in spermatogenesis, implantation, pregnancy and abortion: cross talk and molecular mechanisms. American Journal of Reproductive Immunology 2020; 83(5): e13228, DOI: 10.1111/aji.13228.
27. Perrotta G. The clinical and psychopathological implications in the forms of hyperhistaminosis. Journal of Neurology and Brain Disorders, 2020; 4(3): 347-358.
28. Orazov MR, Radinskiy VY, Khamoshina MB, Nosenko EN, Tokaeva ES, Barsegyan LK et al. Histamine metabolism disorder in pathogenesis of chronic pelvic pain in patients with external genital endometriosis. Patol Fiziol Eksp Ter 2017; 61(2): 56-60.
29. Shrivastav P, Gill DS, Jeremy JY, Craft I, Dandona P. Follicular fluid histamine concentrations in infertile women with pelvic adhesions. Acta Obstetrica Gynecol Scand 1988; 67(8): 727-9.
30. Zhu TH, Zou G, Ding SJ, Li TT, Zhu LB, Wang JZ, Yao YX, Zhang XM. Mast cell stabiliser ketotifen reduces hyperalgesia in a rodent model of surgically induced endometriosis. Journal of Pain Research 2019; 12: 1359-1369.
31. Grundy L, Caldwell A, Caraballo SG, Erickson A, Schober G, Castro J, Harrington AM, Brierley SM. Histamine induces peripheral and central hypersensitivity to bladder distension via the histamine H1 receptor and TRPV1. Renal Physiology 2020; 318(2): F298-F314.
32. Lin HY, Lu JH, Chuang SM, Chueh KS, Juan TJ, Liu YC, Juan YS. Urinary biomarkers in interstitial cystitis/bladder pain syndrome and its impact on therapeutic outcome. Diagnostics 2022; 12 (1): 75.
33. Izquierdo-Casas J, Comas-Baste O, Latorre-Moratalla ML, Lo- rente-Gascon M, Duelo A, Vidal-Carou M et al. Low serum diamine oxidase (DAO) levels in patients with migraine. Journal of Physiology and Biochemistry, 2017; DOI: 10.1007/s13105-017-0571-3.
34. Laurino A, Landucci E, Cinci L, Gencarelli M, De Siena G, Bellusci L et al. Brain histamine modulates the antidepressant-like effect of the 3-iodothyroacetic acid (TA1). Frontiers in Cellular Neurosci- ence 2019; 13: 176, DOI: 10.3389/fncel.2019.00176.
35. Zhang X, Huang Q, Deng Z, Li J, Yan X, Jauhiainen M et al. Dietary cholesterol is essential to mast cell activation and associated obesity and diabetes in mice. Biochim Biophys Acta Mol Basis Dis 2019; 1865(6): 1690-1700.
36. Wang KY, Tanimoto A, Yamada S, Guo X, Ding Y, Watanabe T et al. Histamine regulation in glucose and lipid metabolism via histamine receptors: model for non-alcoholic steatohepatitis in mice. The American Journal of Pathology 2010; 177(2): 713-723.
37. Reese I, Ballmer-Weber B, Beyer K, Dolle-Bierke S, Kleine-Tebbe J, Klimek L et al. Guideline on management of suspected adverse reactions to ingested histamine. Allergologie Select 2021; 5: 305- 314.
38. Pinzer TC, Tietz E, Waldmann E, Schink M, Neurath MF, Zopf Y. Circadian profiling reveals higher histamine plasma levels and lower diamine oxidase serum activities in 24% of patients with suspect- ed histamine intolerance compared to food allergy and controls. Allergy 2018; 73(4): 949-957.
39. Filcek MAM, Vats M, Skrzyniarz-Plutecka A. Discovery of the mechanism of COVID-19, SIRS and SEPSID, defence and treatment. Journal of MAR Pulmonology 2021; 3(5).
40. Jarisch R. Histamine and osteoporosis. Histamine Intolerance 2014; 149: doi: 10.1007/978-3-642-55447-6_11.
41. Sirfuno MM, Suppa M, Ginaldi L et al. Does allergy break bones? Osteoporosis and connection to allergy. Int J Mol Sci 2020; 21: 712.
42. Upfal J, O’Callaghan J. Your medical tests – what do they really mean? Schwartz Publishing, 2001: Melbourne.
43. Sato R, Taguchi M, Nagase H et al. Augmentation of allergic reactions by several pesticides. Toxicicol 1998; 126 (1): 41-53.
44. Genius SJ, Kyrillos E. The chemical disruption of human metabolism. Toxicol Mech Meth 2017; 27 (7): 477-500.
45. Peng H, Wang J, Ye XY et al. Histamine H4 receptor regulates IL-6 and IFN-y secretion in native monocytes from healthy subjects and patients with allergic rhinitis. Clin Transl Aller 2019; 9 (49).
46. Aggarwal P, Senthikumaran S. Dust mite allergy. StatPearls (Inter- net). Treasure Island (FL): StatPearls Publishing 2022.
47. Okuma Y, Okamoto Y, Yonekura S et al. Persistent nasal symptoms and mediator release after continuous pollen exposure in an environmental challenge chamber. Ann Allerg Asthma Immunol 2016; 117(2): 150-7.
48. Theoharides TC, Tsilioni I, Ren H. Recent advances in our understanding of mast cell activation – or should it be mast cell mediator disorders? Expert Rev Clin Immunol 2019; 15 (6): 639-656.